As an optometrist in Fayetteville with over two decades of experience in myopia control, I’ve spoken with countless parents who are understandably concerned about their child's worsening vision. The first question is almost always, "What's their prescription?" While that's important, I guide them to a number that tells a much more critical story about their child's eye health and future: their axial length.
A prescription, measured in diopters, only tells us how to correct vision for today; it doesn't explain why it's changing. Axial length, the physical measurement of the eye from front to back, is the gold standard for tracking myopia. It's the foundation of our sleepSEE® myopia control program right here in Cumberland County because it allows us to address the root cause of progressing nearsightedness.
This article will explain what axial length is, how we measure it, and why it's the key to protecting your child's long-term vision. We'll cover the risks associated with a longer eye and how we can slow its growth.
What is Axial Length, Really?
Myopia occurs when the eye grows too long, causing light to focus in front of the retina instead of on it. This makes distant objects blurry. The longer the eye, the worse the myopia.
Axial length is the physical measurement of that front-to-back distance, in millimeters. While a change in prescription can be influenced by various factors, a change in axial length is a direct, physical measurement of eye growth. This is why it’s so much more accurate. A child's prescription might fluctuate slightly between visits, but the axial length measurement gives us undeniable proof of whether the eye is continuing to elongate at an unhealthy rate.
In our clinic, serving families from Fayetteville to Fort Liberty, axial length measurement is a key part of our myopia control protocol. It allows us to shift from simply correcting blurry vision to proactively managing the underlying issue: excessive eye growth.
How We Measure It: A Look at Optical Biometry
We use an optical biometer to measure axial length. The process is quick, painless, and non-invasive. Your child rests their chin on the machine and looks at a light. A low-power laser scans the eye and provides a measurement in seconds.
This technology is accurate to a hundredth of a millimeter, which is crucial for tracking even small changes in eye growth. This data helps us determine if our treatment strategy is effective.
The Story of Growth: Normal vs. Concerning
While it's normal for a child's eyes to grow, in a myopic child, this growth is accelerated. A non-myopic child's axial length might grow by 0.1 mm per year, while a myopic child might see growth of 0.3 mm or more. This rapid growth is a major red flag.
A 1 mm increase in axial length is equivalent to a prescription change of about -2.50 to -3.00 diopters. This level of change signals the need for intervention.

We use axial length growth charts, much like the height and weight charts at your pediatrician's office, to track your child's eye growth against established data. This allows us to determine if their growth rate is normal or if they are on a trajectory toward high myopia, enabling us to intervene early.
Plotting axial length on a growth chart helps us visualize and track progression against established percentiles. This data makes the concept of 'getting more nearsighted' a measurable reality for parents.
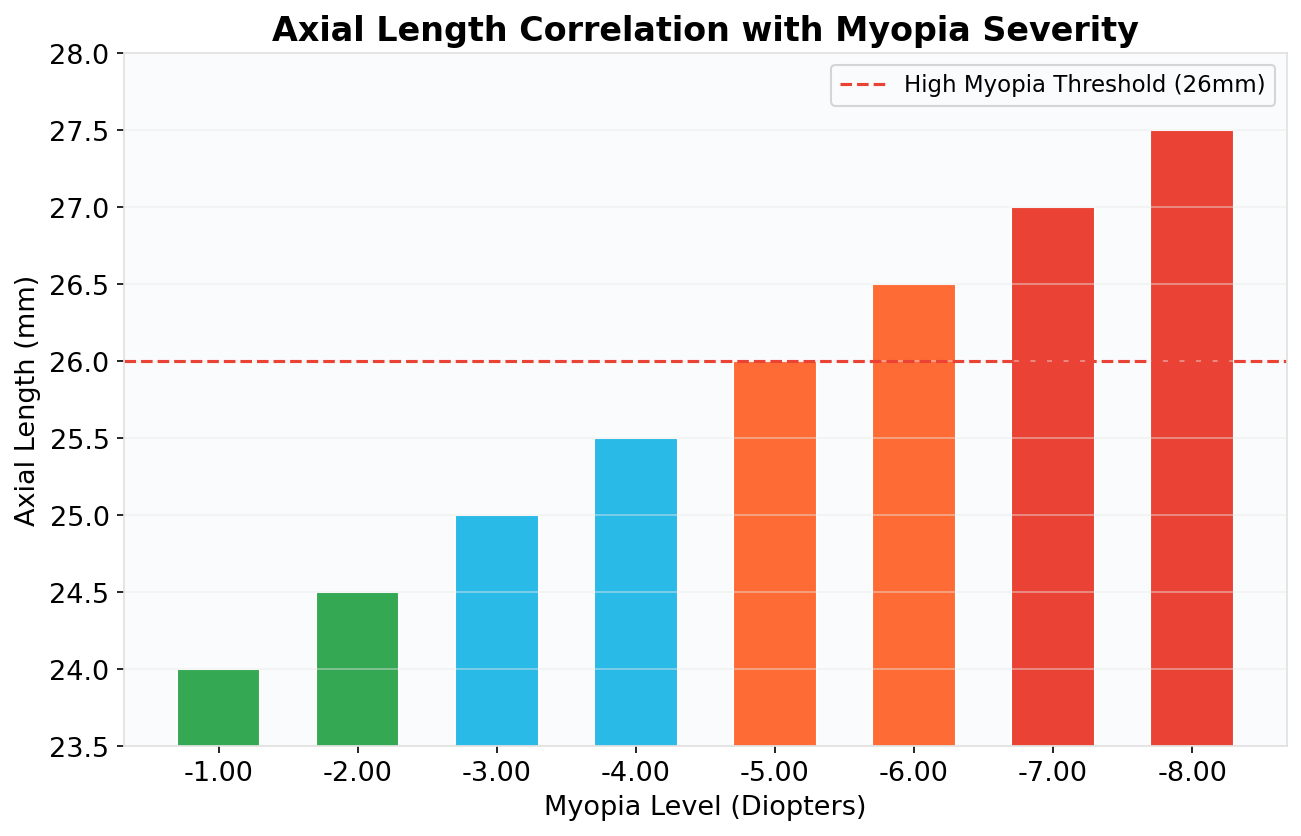
This chart illustrates the direct relationship between the physical length of the eye and the severity of myopia. As the axial length increases, so does the level of nearsightedness, requiring a stronger prescription to achieve clear vision.
The Risks of a Longer Eye: More Than Just Thick Glasses
Uncontrolled myopia is more than an inconvenience. Excessive axial length is a significant risk factor for serious eye diseases later in life. As the eye elongates, the retina and other tissues are stretched and thinned, increasing the risk of:
-
Retinal Detachment: This is a medical emergency. The retina, the light-sensitive tissue at the back of the eye, pulls away from its normal position. This can cause sudden floaters, flashes of light, and a curtain-like shadow over your field of vision. If not treated promptly, it can lead to permanent vision loss.
-
Glaucoma: Often called the "silent thief of sight," glaucoma damages the optic nerve, which connects the eye to the brain. This damage is irreversible and typically starts with the loss of peripheral (side) vision. Many people don't notice the changes until the damage is significant. High myopia is a major risk factor for developing glaucoma.
-
Myopic Maculopathy: This condition affects the macula, the central part of the retina responsible for sharp, detailed vision. As the eye stretches, the macula can thin and degenerate, leading to distorted or blurry central vision. This can make activities like reading, driving, and recognizing faces difficult.
-
Cataracts: While cataracts are a common part of aging, high myopia can cause them to develop earlier in life. A cataract is a clouding of the eye's natural lens, which can make vision blurry, hazy, or less colorful.
-
Retinal Detachment: A sight-threatening emergency where the retina pulls away from its normal position.
-
Glaucoma: A disease that damages the optic nerve, leading to irreversible peripheral vision loss.
-
Myopic Maculopathy: A leading cause of vision loss in highly myopic eyes, where the central part of the retina degenerates.
-
Cataracts: A clouding of the eye's lens that can occur earlier in life in people with high myopia.
Studies from the American Academy of Ophthalmology show that a person with a -6.00 diopter prescription has a 22 times higher risk of retinal detachment and a 40 times higher risk of myopic maculopathy. These risks are directly tied to axial length.
| Axial Length (mm) | Approximate Myopia | Lifetime Risk of Visual Impairment |
|---|---|---|
| < 26 mm | Low to Moderate Myopia | Low (3-5%) |
| 26 to 28 mm | High Myopia | Moderate (25-35%) |
| > 28 mm | Extreme Myopia | High to Very High (50-90%) |
This is why our mission in myopia control is not just about clear vision for your child today; it's about preserving their eye health and preventing vision loss for the rest of their lives. It’s a preventative healthcare strategy for their eyes.
How sleepSEE® Ortho-K Puts the Brakes on Growth
Yes, we can do something about it. Orthokeratology (Ortho-K), the cornerstone of our sleepSEE® program, involves wearing custom-designed contact lenses overnight. These lenses gently reshape the cornea while you sleep, providing clear vision during the day without glasses or contacts.
The real magic of Ortho-K is how it affects eye growth. When a child wears standard glasses or contact lenses, the central vision is corrected, but the peripheral vision is not. This creates a phenomenon called 'peripheral hyperopic defocus,' where light focuses behind the peripheral retina. It's believed that this sends a signal to the eye to keep growing longer to 'catch up' to the light. Ortho-K, on the other hand, reshapes the cornea in such a way that it creates 'peripheral myopic defocus.' This means that light focuses in front of the peripheral retina. This is thought to send a 'stop' signal to the eye, which slows down the drive for axial elongation. [1] It's a subtle but powerful change in the eye's optics that has a profound effect on its growth.
Studies have shown that Ortho-K can slow axial length growth in myopic children by 50% or more compared to glasses. [2] This reduces the final prescription and the lifetime risk of eye disease.
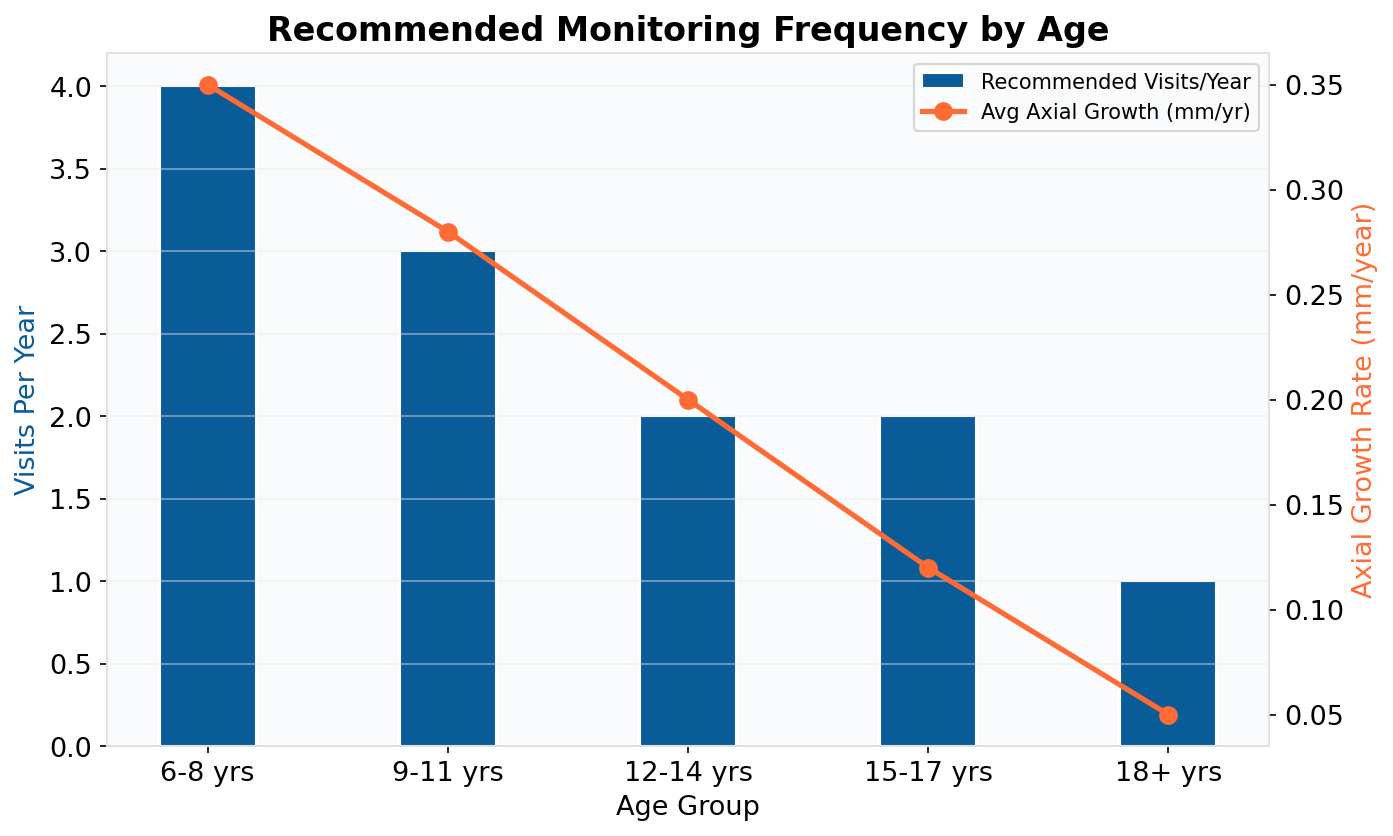
Effective myopia control relies on consistent monitoring. This chart outlines our recommended frequency for axial length measurements based on a child's age, ensuring we track growth closely during the most critical periods of progression.
Investing in a Lifetime of Healthy Sight
sleepSEE® myopia control is a specialty service not covered by insurance. Flexible payment options and HSA/FSA funds are accepted. This investment in your child's eye health is crucial. By focusing on axial elongation, we are working to protect your child's future vision.
Is your child a candidate for our sleepSEE® program? Take our online candidacy quiz [blocked] to find out. Learn more on our how it works [blocked] page and our blog [blocked].
My goal is to provide the best care to my community. Using axial length measurement and treatments like Ortho-K allows me to focus on what truly matters: a lifetime of healthy sight.
Frequently Asked Questions
Is the axial length measurement painful for my child?
No, the measurement is taken with a non-contact optical biometer. It's painless, quick, and involves no eye drops or puffs of air.
Why doesn't my regular family eye doctor measure axial length?
Axial length measurement requires an optical biometer, which is not yet standard in all eye care practices. It is typically found in specialty clinics focused on myopia control.
What is a "normal" axial length?
Normal axial length varies by age. More important than a single number is the rate of change. We use growth charts to determine if a child's eye growth is accelerated, which indicates the need for treatment.
Can Ortho-K or other treatments reverse or shorten the axial length?
The primary goal of Ortho-K is not to reverse growth but to significantly slow down the rate of future elongation. This reduces the final level of myopia and associated risks.
What if my child plays sports? Can they still do Ortho-K?
Absolutely! Ortho-K is an excellent option for active children and teens. Since the lenses are only worn at night, your child will have clear vision all day long without needing to worry about glasses breaking or contact lenses falling out during sports or other activities. It provides a level of freedom that many young athletes and their parents appreciate.
How often does my child need to be monitored?
We recommend axial length measurements every 6 months for children ages 6-12 and every 12 months for older teens. Consistent monitoring is key to effective treatment.
Last reviewed: February 2026
References
[1] Chen, Z., et al. (2016). Effects of orthokeratology on choroidal thickness and axial length. Optometry and Vision Science.
[2] Zhu, M. J., et al. (2014). The control effect of orthokeratology on axial length elongation in Chinese children with myopia. BMC ophthalmology.
Free Download: The Science Behind Ortho-K
A plain-language summary of 12 key clinical studies on orthokeratology efficacy.
- Summary of 12 peer-reviewed clinical studies
- Myopia progression rates with/without treatment
- Ortho-K vs. atropine vs. multifocal lenses
- FDA approval history and safety data
Ortho-K Research Summary
Science & Evidence — Free PDF
sleepSEE Medical Advisory Board
sleepSEE Medical Advisory Board is a contributor to the sleepSEE Insights blog, sharing expert knowledge on myopia progression, orthokeratology (Ortho-K) and myopia control.