As a dad and an optometrist here in Fayetteville, I get a lot of questions from parents who are worried about their child’s eyesight. They see their kid’s glasses getting thicker every year and they ask me, “Dr. Singletary, is there anything we can do to stop this?” It’s a question that hits close to home, especially with so many of our local families serving at Fort Liberty or navigating the Cumberland County school system. You want your kids to have every advantage, and clear, healthy vision is a big part of that.
Here’s the thing: for a long time, the answer was just stronger glasses. But now, we have incredible options for Myopia Control that can actually slow down the progression of nearsightedness in children. Two of the most effective and popular methods we use in my practice are Ortho-K, which we call sleepSEE®, and low-dose atropine eye drops.
So, which one is the right choice for your child? That’s the million-dollar question, isn’t it? Let me break it down for you, parent to parent, so you can feel confident in making the best decision for your family.
In This Article
- Ortho-K vs. Atropine Drops: Which Myopia Control Method Is Right for Your Child?
- What is Myopia, and Why Should We Care?
- The sleepSEE® Solution: Ortho-K Lenses
- The Atropine Option: Medicated Eye Drops
- Head-to-Head: Ortho-K vs. Atropine
- Making the Decision: What’s Right for Your Fayetteville Family?
- A Note on Insurance and Cost
- Frequently Asked Questions
- Let’s Protect Your Child’s Vision Together
What is Myopia, and Why Should We Care?
Before we dive into the solutions, let’s get on the same page about the problem. Myopia is the medical term for nearsightedness. It means your child can see things up close just fine, but things farther away—like the whiteboard at school or the baseball they’re supposed to be catching—are blurry. This happens because the eyeball grows too long, causing light to focus in front of the retina instead of directly on it.
A little bit of myopia isn’t a big deal. But when it progresses, it’s not just about needing thicker glasses. High myopia significantly increases the risk of serious, sight-threatening eye diseases later in life, like retinal detachment, glaucoma, and myopic maculopathy. That’s why we’ve shifted from just correcting vision to actively controlling myopia progression. It’s about protecting your child’s future eye health.
The sleepSEE® Solution: Ortho-K Lenses
Ortho-K is a remarkable technology that we’ve branded as sleepSEE® in our practice. It stands for orthokeratology, and it’s a non-surgical treatment that uses specially designed rigid contact lenses to gently and temporarily reshape the cornea overnight. Think of it like a retainer for the eye.
Your child wears the lenses while they sleep, and in the morning, they take them out and can see clearly all day long without any glasses or daytime contacts. It’s a game-changer for active kids, especially those in sports or who just hate the hassle of glasses. No more worrying about broken frames during a soccer game or losing a contact lens in the pool.

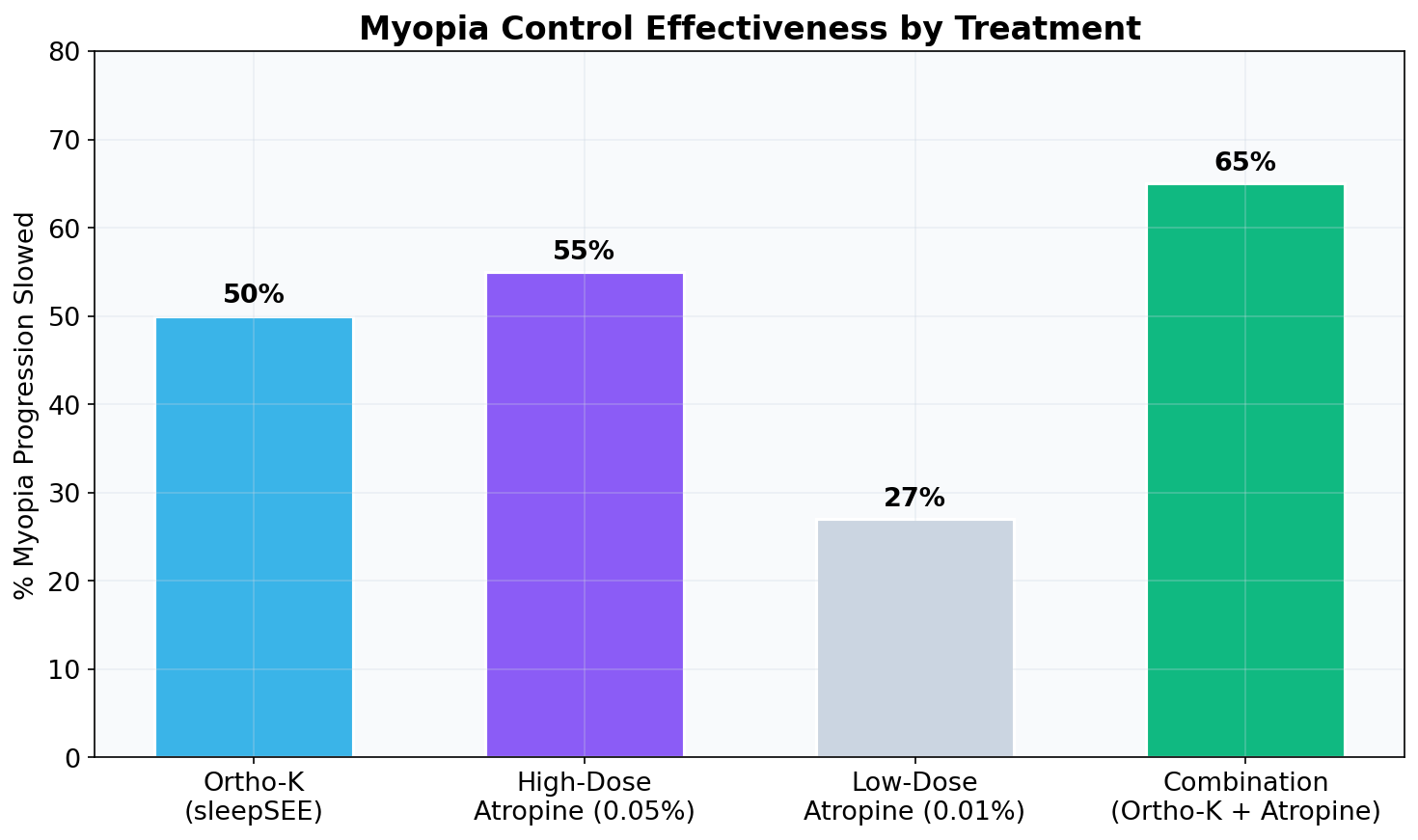
But here’s the most important part: it’s not just about clear vision. The way Ortho-K reshapes the cornea also changes how light focuses on the peripheral retina. This peripheral defocus is believed to be the key mechanism that signals the eye to stop growing longer, thereby slowing down myopia progression. Studies have shown that Ortho-K can slow myopia progression by 30-60% in many children. [1]
Pros of sleepSEE® (Ortho-K):
- Freedom from Daytime Glasses/Contacts: This is the biggest lifestyle benefit.
- Proven Myopia Control: Strong clinical evidence shows it effectively slows myopia progression.
- Reversible: The corneal reshaping is temporary. If your child stops wearing the lenses, their cornea and prescription will return to their original state.
Cons of sleepSEE® (Ortho-K):
- Hygiene and Responsibility: Requires diligent cleaning and handling of the lenses every night. It’s a commitment for both the child and the parents.
- Initial Adaptation: There can be a short adjustment period as your child gets used to the feeling of the lenses.
- Cost: This is a specialty service, which I'll discuss more in a bit.
The Atropine Option: Medicated Eye Drops
Another powerful tool we have for Myopia Control is low-dose atropine eye drops. This isn’t a new medication—optometrists have used atropine for decades for various purposes. What’s new is using it in a very diluted form (typically 0.01% to 0.05%) specifically to slow down myopia.
Unlike Ortho-K, atropine doesn’t correct your child’s vision. It’s purely a therapeutic treatment. Your child will still need to wear their regular glasses or contact lenses during the day to see clearly. The treatment involves putting one drop in each eye every night before bed. It’s simple, non-invasive, and can be a great option for younger children or those who aren’t ready for contact lenses.

The exact way atropine works to slow eye growth isn’t fully understood, but research suggests it involves receptors in the retina and sclera (the white part of the eye) that influence the eye’s growth signals. The effectiveness is well-documented; studies have shown that low-dose atropine can reduce myopia progression by 50-60%, which is comparable to Ortho-K. [2]
Pros of Atropine Drops:
- Easy to Use: Administering eye drops is straightforward for most parents.
- Non-Invasive: No contact lenses are involved.
- Effective: Clinically proven to significantly slow myopia progression.
Cons of Atropine Drops:
- Still Need Glasses: Does not provide vision correction, so glasses or contacts are still required during the day.
- Potential Side Effects: Though minimal at low doses, some children experience light sensitivity (from slightly larger pupils) and difficulty with up-close focusing. We monitor this closely.
- Consistency is Key: The drops must be used every single night to be effective.
Head-to-Head: Ortho-K vs. Atropine
So, how do these two leading treatments stack up against each other? Both are fantastic options, and the truth is, there isn't one single "best" choice for every child. It really comes down to a personalized decision based on your child's specific needs, your family's lifestyle, and our clinical findings.
Let's look at the data. When we compare the effectiveness, both treatments show significant success in slowing down the rate of eye growth. A 2023 meta-analysis published in Optometry and Vision Science confirmed that both Ortho-K and low-dose atropine have similar efficacy in myopia control. [3]
Of course, effectiveness is only part of the story. We also have to consider the potential side effects. Both treatments are very safe, but it's important to be aware of the differences.
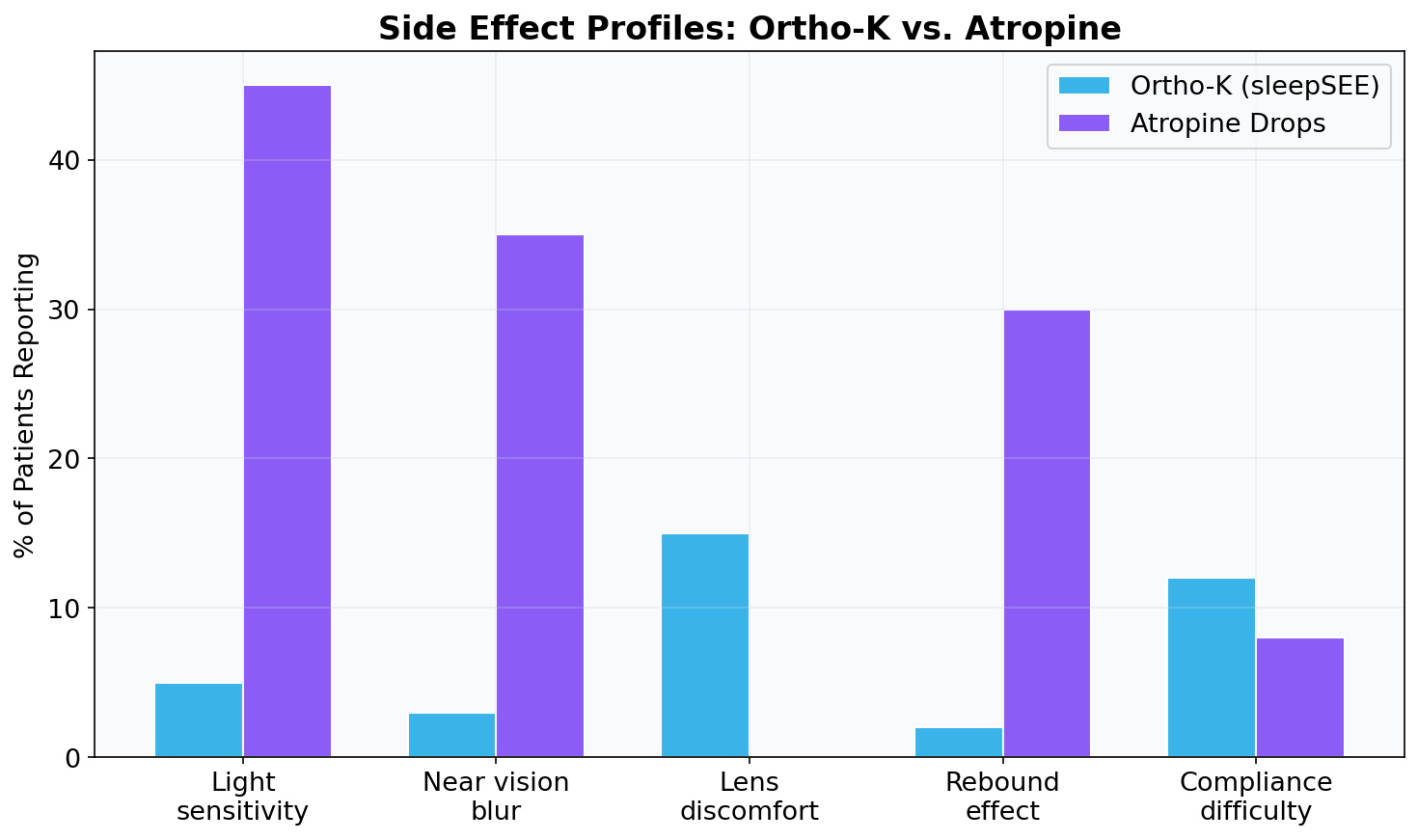
As you can see, the side effect profiles are quite different. With sleepSEE®, the primary concerns are related to contact lens wear—things like dryness or irritation, which are usually minor and manageable. With atropine, the side effects are related to the medication itself, like light sensitivity. We can often manage this by having your child wear sunglasses outdoors or by adjusting the dosage.
For a deeper dive into all the options, you can read our Complete Guide to Myopia Control Options Compared [blocked].
Making the Decision: What’s Right for Your Fayetteville Family?
Here in our Fayetteville practice, I’ve helped hundreds of families navigate this decision. For a family with a 10-year-old who plays travel soccer and spends weekends at the lake, the freedom of sleepSEE® is often a perfect fit. For a younger, more timid 7-year-old, starting with atropine drops might feel less intimidating.
We also consider our many military families from Fort Liberty. With the potential for moves and changing schools, having a Myopia Control plan that is consistent and effective is key. Both sleepSEE® and atropine are excellent for this, and we work with families to ensure continuity of care, even if they get stationed elsewhere.
Here’s the thing, there’s even a third option: combination therapy. For some children with very rapidly progressing myopia, we may recommend using both sleepSEE® and atropine drops together. Research published in journals like the Journal of the American Medical Association (JAMA) Ophthalmology has shown this combination can be even more effective than either treatment alone. [4]
A Note on Insurance and Cost
This is a really important point I want to be upfront about. sleepSEE® myopia control is a specialty service not covered by insurance. This includes plans common in our area like TRICARE and Blue Cross. Why? Because insurance companies currently classify myopia control as an elective or “cosmetic” service, similar to LASIK, rather than a medical necessity. We all know that’s not true—preventing future eye disease is absolutely a medical necessity!—but that’s the reality of the system for now.
We are strong advocates for changing this, but in the meantime, we are committed to making this care affordable. We offer flexible payment options and accept HSA/FSA funds to help families budget for this important investment in their child’s future.
Frequently Asked Questions
1. How old does my child need to be to start Myopia Control?
Generally, we can start Myopia Control as soon as we detect myopia progression, often around age 6 or 7. The earlier we start, the more impact we can have on slowing down the progression.
2. Are these treatments safe?
Yes, both Ortho-K and low-dose atropine have been extensively studied and are considered very safe when administered and monitored by a qualified optometrist. We follow strict safety protocols in our practice.
3. How long will my child need to be in treatment?
Myopia typically stabilizes in the late teens or early twenties. We generally continue treatment until we see that your child’s prescription has remained stable for at least a year or two.
4. What if my child is scared of eye drops or contact lenses?
This is a very common concern! We have a lot of experience helping kids feel comfortable. For sleepSEE®, we do a very thorough training session. For atropine, we can show you techniques to make it a quick and stress-free part of the nightly routine.
5. Can my child switch treatments if one isn’t working out?
Absolutely. The great thing about these options is that they are flexible. If one treatment isn’t a good fit for lifestyle or other reasons, we can often switch to the other. The most important thing is to have a plan in place.
6. Where can I learn more about how overnight lenses work?
We have another article that goes into more detail here: How Overnight Contact Lenses Control Myopia [blocked].
Let’s Protect Your Child’s Vision Together
Choosing a Myopia Control plan is a big decision, but it’s one of the most important you can make for your child’s long-term eye health. I hope this breakdown has been helpful. The next step is to come in for a comprehensive myopia evaluation so we can determine the best path forward for your child.
By Dr. James Singletary, OD, FIAOMC
Last reviewed: February 2026
References:
[1] Sun, Y., Xu, F., Zhang, T., Liu, M., Wang, D., Chen, Y., & Liu, Q. (2015). Orthokeratology to control myopia in children: a meta-analysis. Optometry and Vision Science, 92(3), 252-257. https://pubmed.ncbi.nlm.nih.gov/25692857/
[2] Yam, J. C., Jiang, Y., Tang, S. M., Law, A. K. P., Chan, J. J., Wong, E., ... & Yip, B. H. K. (2019). Low-concentration atropine for myopia progression (LAMP) study: a randomized, double-blinded, placebo-controlled trial of 0.05%, 0.025%, and 0.01% atropine eye drops in myopia control. Ophthalmology, 126(1), 113-124. https://www.aaojournal.org/article/S0161-6420(18)30792-5/fulltext
[3] Tsai, H. R., Wang, J. H., & Chiu, C. J. (2023). Efficacy of atropine, orthokeratology, and combined treatment in slowing myopia progression: a systematic review and meta-analysis. Optometry and Vision Science, 100(1), 14-25. https://pubmed.ncbi.nlm.nih.gov/35688780/
[4] Tan, Q., Ng, A. L. K., Choy, B. N. K., & Cheng, G. P. M. (2023). Combined 0.01% Atropine with Orthokeratology in Childhood Myopia Control (AOK) Study: A 2-Year Randomized Clinical Trial. JAMA Ophthalmology, 141(3), 220–227. https://jamanetwork.com/journals/jamaophthalmology/fullarticle/2800536
External Resources:
Ortho-K vs. Atropine Drops: Side-by-Side
A direct comparison of the two most clinically studied myopia control treatments for children.
| Feature | Ortho-K (sleepSEE)★ Recommended | Atropine Eye Drops |
|---|---|---|
| Myopia Slowed | Up to 50% | Up to 77% (0.01% dose) |
| Glasses-Free During Day | Yes | No |
| How Used | Wear lenses at night | 1 drop nightly |
| Side Effects | Minimal (adaptation period) | Light sensitivity, blurred near vision |
| FDA Status | Yes | Off-label use |
| Best For | Active kids, sports, convenience | Younger children, high progression |
| Avg. Annual Cost | $1,200–$1,800 | $300–$600 |
| Reversible | Yes | Yes |
Many specialists combine ortho-k with low-dose atropine for maximum effect. Ask your provider about combination therapy.
Find a sleepSEE Certified ProviderFree Download: Myopia Risk Checklist for Parents
Is your child's vision at risk? Get the 10-point checklist used by ortho-k specialists.
- 10 warning signs myopia is progressing
- Questions to ask your eye doctor
- How to evaluate ortho-k candidacy
- What to expect in the first 30 days
Myopia Risk Checklist
For Parents — Free PDF Guide
Dr. James Singletary, OD, FIAOMC
Dr. James Singletary, OD, FIAOMC is a contributor to the sleepSEE Insights blog, sharing expert knowledge on myopia progression, orthokeratology (Ortho-K) and myopia control.