Last reviewed: February 2026 by the sleepSEE Clinical Advisory Team
In This Article
- What Is Orthokeratology?
- Who Is a Good Candidate?
- Age: When Can a Child Start?
- Prescription Range: What Qualifies?
- Lifestyle Fit: Is Your Child Ready?
- Who May Not Be a Candidate
- The Candidacy Evaluation Process
- sleepSEE vs. Other Myopia Control Options
- What Parents in Fayetteville Are Asking
- Frequently Asked Questions
- The Bottom Line
Every week, parents sit across from me in the exam room and ask the same question: "Is my child a good candidate for ortho-k?"
It's a great question. And honestly, more children qualify than most parents expect.
But candidacy isn't one-size-fits-all. There are real criteria — prescription range, corneal shape, age, lifestyle — that determine whether orthokeratology is the right fit. This guide walks you through all of them, so you can walk into your child's next eye exam with the right questions ready.
What Is Orthokeratology?
Orthokeratology — or ortho-k — uses custom-designed, FDA-approved rigid gas-permeable lenses worn overnight. While your child sleeps, the lenses gently reshape the front surface of the eye (the cornea). By morning, the cornea holds a new shape that focuses light correctly. The lenses come out, and your child sees clearly all day — no glasses, no daytime contacts.
For children with myopia (nearsightedness), ortho-k does two things at once: it corrects vision and slows the progression of myopia. That second benefit is why so many eye doctors — including our team at Eye Medics Optometry in Fayetteville, NC [blocked] — recommend it for children over standard glasses.
A consultation at Eye Medics Optometry — the first step in determining if your child is a candidate.
Who Is a Good Candidate?
Candidacy depends on four main factors: age, prescription strength, corneal health, and lifestyle readiness. Let's break each one down.
Age: When Can a Child Start?
The FDA has approved ortho-k lenses for children as young as 6 years old. In practice, most children between 6 and 17 are excellent candidates — and the earlier they start, the more myopia progression they can prevent.
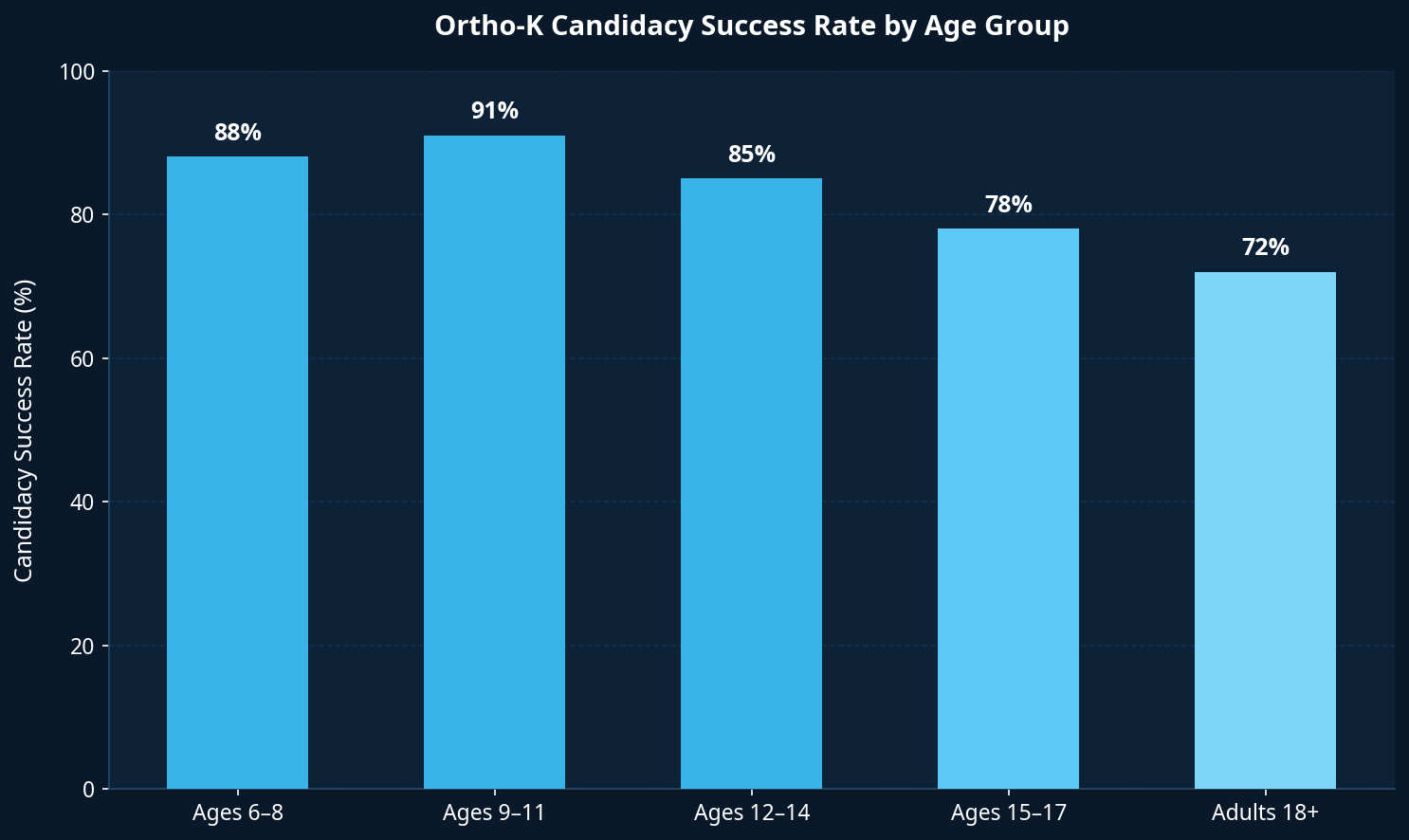
Why does starting early matter so much? Because myopia progresses fastest between ages 6 and 12. Every diopter of myopia that develops during this window increases the lifetime risk of serious eye conditions — including retinal detachment, glaucoma, and myopic maculopathy. [1]
Starting ortho-k at age 7 instead of age 12 means five fewer years of unchecked progression. That's a meaningful difference in long-term eye health.
Prescription Range: What Qualifies?
Ortho-k is most effective for children with mild to moderate myopia — typically in the range of -0.50 to -6.00 diopters (D). Some providers can fit prescriptions up to -8.00 D, though results may vary at higher levels.
Astigmatism up to about -1.75 D can also be corrected with ortho-k lenses, though higher amounts may require a different approach.
| Prescription Range | Ortho-K Suitability |
|---|---|
| -0.50 to -3.00 D | Excellent — full correction typically achieved |
| -3.00 to -6.00 D | Good — most patients achieve functional daytime vision |
| -6.00 to -8.00 D | Possible — partial correction; discuss with your provider |
| Above -8.00 D | Generally not recommended for ortho-k alone |
| Astigmatism ≤ -1.75 D | Treatable with toric ortho-k designs |
If your child's prescription falls outside the ideal range, your provider may recommend combining ortho-k with low-dose atropine drops for enhanced myopia control.
Lifestyle Fit: Is Your Child Ready?
Ortho-k requires a nightly routine. Your child needs to:
- Insert lenses before bed (takes about 5 minutes once learned)
- Sleep with the lenses in for 6–8 hours
- Remove lenses in the morning and store them properly
- Clean and disinfect lenses daily
Most children 8 and older can manage this routine with minimal parental help after the first few weeks. Younger children (ages 6–7) typically need a parent to assist with insertion and removal.
Responsibility matters here. If your child regularly loses glasses or forgets homework, that's worth discussing with your provider — not as a disqualifier, but as a factor in planning the right support system.

Who May Not Be a Candidate?
Ortho-k is safe for the vast majority of children, but there are some situations where it may not be the best fit:
- Active eye infections or chronic dry eye — these need to be treated first
- Keratoconus or irregular corneal shape — requires specialized fitting or a different treatment
- Prescription above -8.00 D — may not achieve adequate daytime correction
- Severe allergies affecting the eyes — may cause discomfort with lens wear
- Inability or unwillingness to follow the nightly routine — compliance is essential for results
None of these are permanent disqualifiers. Many can be addressed with treatment or a modified approach. The candidacy evaluation will identify any concerns.
The Candidacy Evaluation Process
A candidacy evaluation at Eye Medics Optometry in Fayetteville takes about 60–90 minutes and includes:
- Comprehensive eye exam — checking vision, prescription, and eye health
- Corneal topography — a painless scan that maps the shape of your child's cornea (this is the key measurement for custom lens design)
- Tear film assessment — checking that the eye produces enough tears for comfortable lens wear
- Discussion of goals and expectations — we want to understand what your child and your family are hoping to achieve
If your child qualifies, lenses are custom-designed based on the corneal topography data. Most families receive their first pair of lenses within 1–2 weeks.
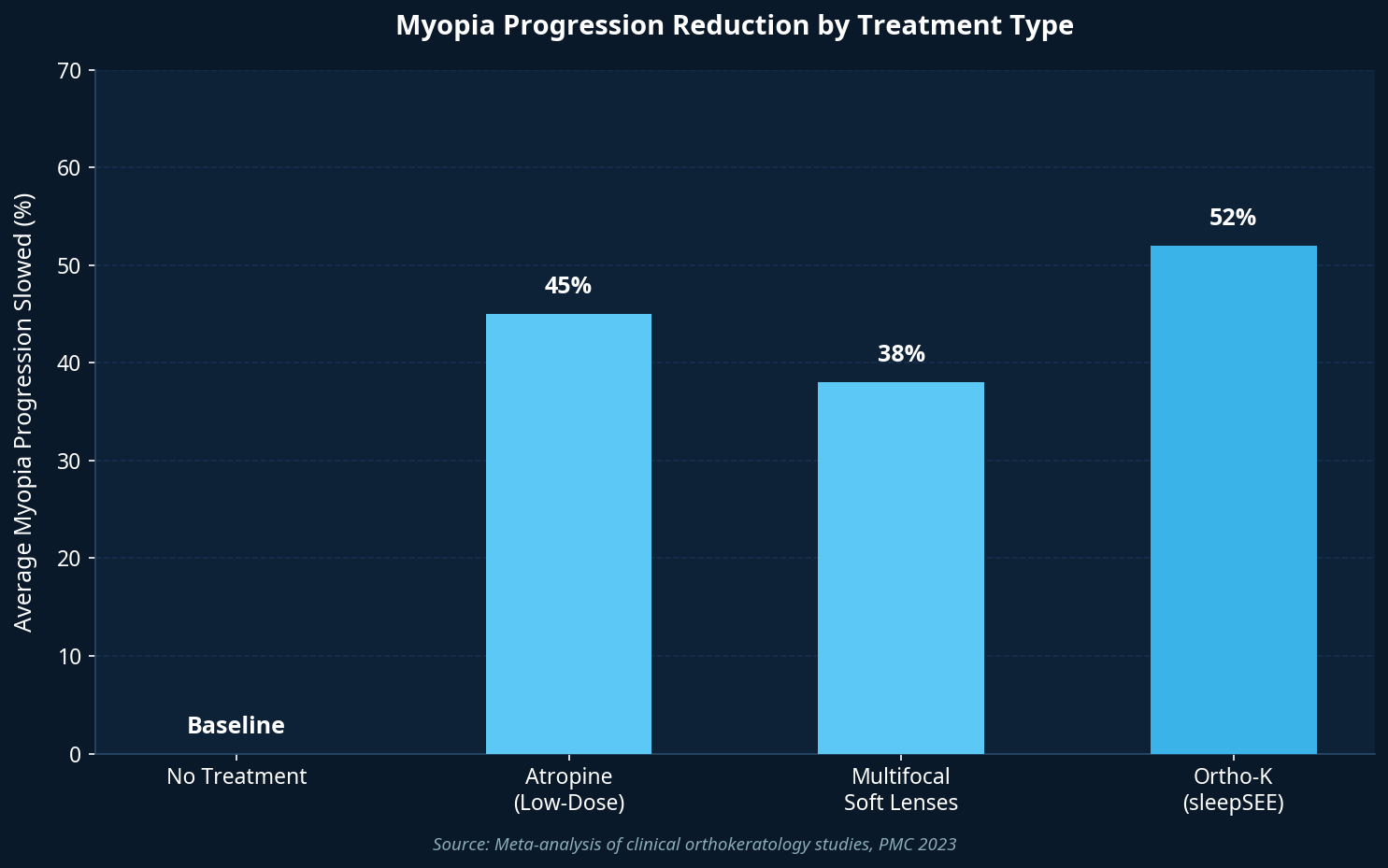
sleepSEE vs. Other Myopia Control Options
Ortho-k isn't the only myopia control treatment available, but it offers a unique combination of benefits. Here's how it compares:
| Treatment | Progression Reduction | Daytime Vision | Age Range | Reversible |
|---|---|---|---|---|
| sleepSEE (Ortho-K) | 36–56% | Clear without correction | 6+ | Yes |
| Low-dose Atropine | 40–60% | Requires glasses/contacts | 5+ | Yes |
| Multifocal Soft Lenses | 30–45% | Requires daytime lenses | 8+ | Yes |
| Standard Glasses | 0% | Corrects only | Any | N/A |
For active children — especially those in sports, swimming, or activities where glasses are a nuisance — ortho-k's glasses-free days are a significant quality-of-life advantage. For families at Fort Liberty and throughout Cumberland County, where children are often involved in youth sports leagues and outdoor activities, this matters a lot.
What Parents in Fayetteville Are Asking
Parents across Fayetteville, Hope Mills, Spring Lake, and the Fort Liberty community have been asking about ortho-k in growing numbers. Here are the questions I hear most often at Eye Medics Optometry:
"My child's prescription keeps getting stronger every year. Will ortho-k stop that?" It won't stop progression entirely, but it significantly slows it. Most children on ortho-k see 40–56% less progression compared to glasses alone.
"My child is only 7. Isn't that too young?" Not at all. Age 6 and up is FDA-approved, and starting earlier means more years of protection during the fastest-progressing window of childhood.
"We're a military family and move every 2–3 years. Can we continue ortho-k at our next duty station?" Yes. sleepSEE providers are located across the country, and your child's corneal topography maps and lens parameters travel with you. Transitions are straightforward.
"What happens if my child decides to stop?" The cornea returns to its original shape within 1–4 weeks. There are no permanent changes to the eye.

Frequently Asked Questions
Q: Does insurance cover ortho-k? sleepSEE® myopia control is a specialty service not covered by insurance. Flexible payment options and HSA/FSA funds are accepted. Many families find that the investment compares favorably to years of glasses, replacement frames, and prescription updates.
Q: How long does it take to see results? Most children notice improved vision after the first night. Full correction typically takes 7–14 days. Some children with higher prescriptions may take 3–4 weeks to reach their target vision.
Q: Are the lenses comfortable? Ortho-k lenses are worn during sleep, so comfort during wear is rarely an issue. Insertion and removal take practice — most children are comfortable with the routine within 2 weeks.
Q: What if the lenses don't fit correctly? Custom lenses are adjusted as needed during the fitting process. Follow-up visits at 1 day, 1 week, and 1 month after fitting allow your provider to fine-tune the fit.
Q: Can both eyes have different prescriptions? Yes. Each lens is custom-made for each eye independently.
Q: How do I know if my child's myopia is progressing fast enough to warrant treatment? Any measurable progression from one year to the next is a reason to consider myopia control. You don't need to wait until the prescription is "high enough" — earlier intervention produces better outcomes.
The Bottom Line
Most children with myopia between -0.50 and -6.00 D, ages 6 and up, are candidates for orthokeratology. The evaluation is straightforward, the treatment is reversible, and the long-term benefits for eye health are well-documented.
If your child's prescription is getting stronger each year, the best time to act is now — not when it gets worse.
Check Your Child's Candidacy [blocked] | Find a sleepSEE Provider Near You [blocked]
Last reviewed: February 2026 | Sources: [1] PMC — Myopia and Associated Pathological Complications | [2] JAMA Ophthalmology — Myopia Control Interventions
Free Download: Myopia Risk Checklist for Parents
Is your child's vision at risk? Get the 10-point checklist used by ortho-k specialists.
- 10 warning signs myopia is progressing
- Questions to ask your eye doctor
- How to evaluate ortho-k candidacy
- What to expect in the first 30 days
Myopia Risk Checklist
For Parents — Free PDF Guide
sleepSEE Medical Advisory Board
sleepSEE Medical Advisory Board is a contributor to the sleepSEE Insights blog, sharing expert knowledge on myopia progression, orthokeratology (Ortho-K) and myopia control.