I want to start with something I see almost every week in my practice.
A parent brings in their 8-year-old. The child has been squinting at the board at school. We run the exam, and sure enough — myopia. Nearsightedness. The parent says, "Okay, we'll get glasses." And I have to gently explain that glasses are only part of the answer.
Here's the thing most parents don't know: myopia isn't just a vision problem. It's a growth problem. The eyeball is physically getting too long. And if we don't do something to slow that growth down, it keeps going — year after year — until that child is a teenager with a prescription so strong they can barely function without correction.
Table of Contents
- What Is Myopia — and Why Should Parents Worry?
- The Numbers Are Alarming
- The Long-Term Risks Nobody Talks About
- Why Is This Happening So Fast?
- How sleepSEE Overnight Lenses Work
- sleepSEE vs. Glasses: Side-by-Side
- When Should You Start?
- Frequently Asked Questions
What Is Myopia — and Why Should Parents Worry? {#what-is-myopia}
Myopia means your child can see things up close just fine, but anything across the room is blurry. It happens because the eyeball grows too long from front to back. Light ends up focusing in front of the retina instead of directly on it. Simple enough to understand. The harder part? Once it starts, it rarely stops on its own.
For families here in Fayetteville — and for the many military families stationed at Fort Liberty — this is especially important. Active-duty life means frequent moves, new schools, new eye doctors. A child whose myopia is quietly progressing can fall through the cracks. That's why I always tell parents: don't wait for the school nurse to flag it. Come in.
The Numbers Are Alarming {#the-numbers}
This isn't a small problem. Globally, myopia affects roughly 30% of the world's population — and that number is expected to reach 50% by 2050, according to a landmark projection published in Ophthalmology by Holden et al. (2016). In the United States, the American Optometric Association estimates that 42% of Americans between ages 12 and 54 are already myopic, up from just 25% in the 1970s.
Here in North Carolina, we're seeing the same trend. Cumberland County schools have seen a noticeable uptick in children needing vision correction over the past decade. I'm not just citing statistics here. I'm seeing it in my chair.
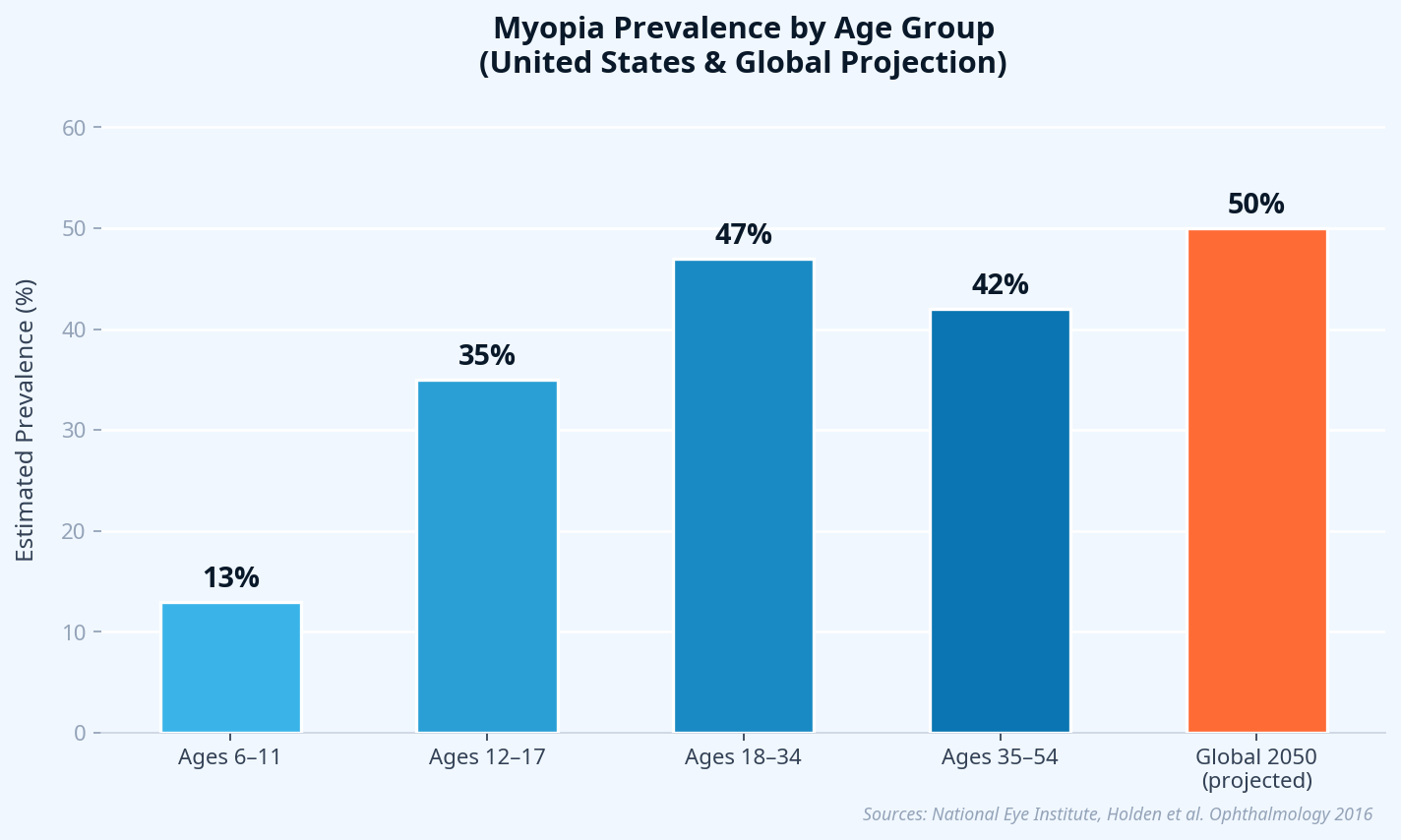
Sources: National Eye Institute; Holden BA, et al. Ophthalmology. 2016.
The Long-Term Risks Nobody Talks About {#long-term-risks}
This is where the conversation gets serious.
High myopia — a prescription of -6.00 diopters or more — isn't just "really nearsighted." It significantly increases the lifetime risk of several blinding conditions. A 2019 meta-analysis published in JAMA Ophthalmology found that high myopia is associated with a 7–8× increased risk of retinal detachment, a 3× increased risk of glaucoma, and a 40× increased risk of myopic maculopathy compared to non-myopic eyes.
Let me put that in plain terms: the thicker your child's glasses get, the higher their risk of serious eye disease later in life. That's why we don't just want to correct myopia — we want to control it.
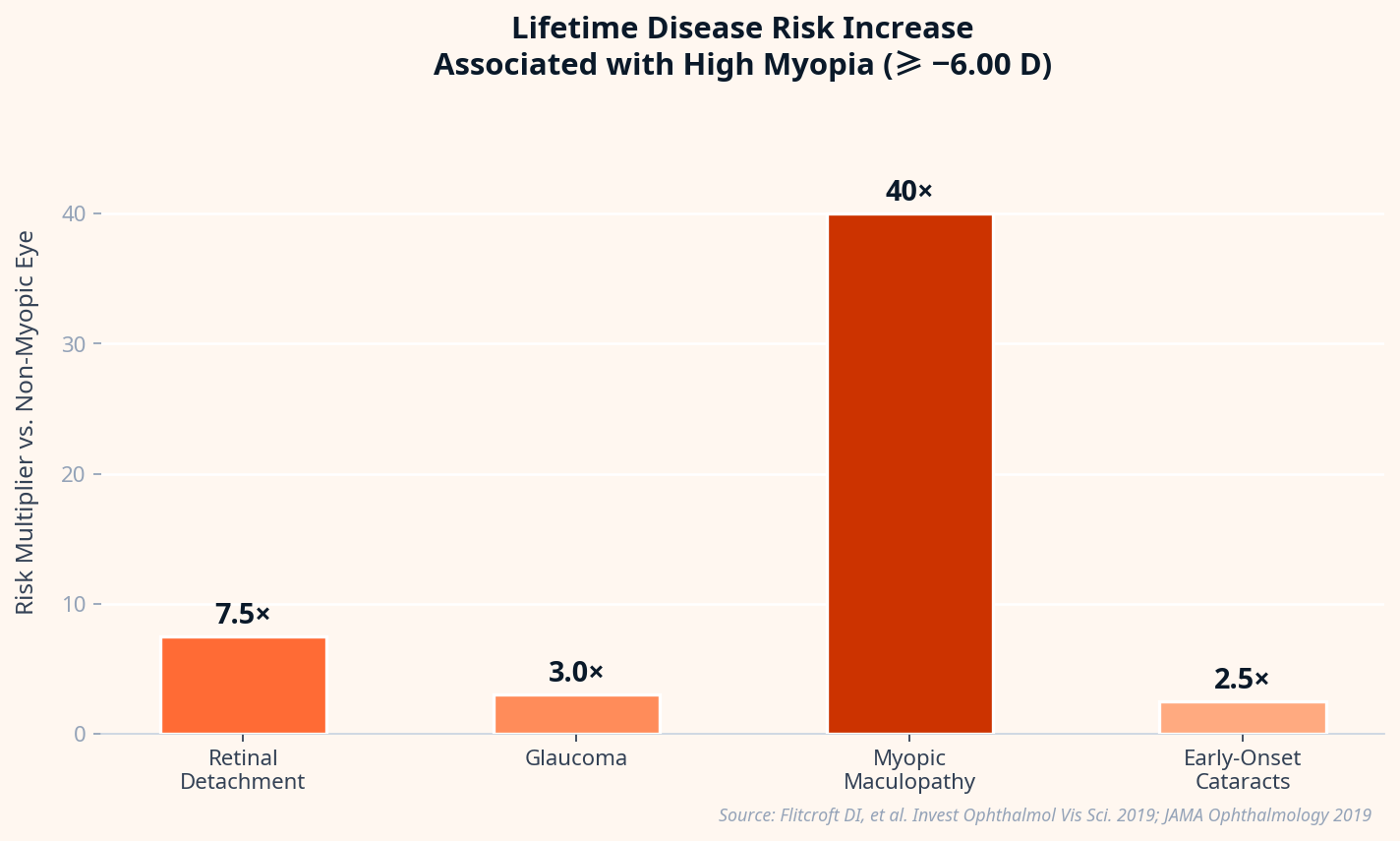
Source: Flitcroft DI, et al. Invest Ophthalmol Vis Sci. 2019; JAMA Ophthalmology 2019.
Why Is This Happening So Fast? {#why-happening}
Honestly? Screens and walls.
Children today spend far less time outdoors and far more time doing near work — reading, tablets, phones, homework. Research consistently shows that time outdoors is one of the strongest protective factors against myopia development. A study published in JAMA Ophthalmology found that each additional hour per week of outdoor time reduced myopia risk by about 2%.
The biology behind it: when a child focuses up close for hours at a stretch, the eye receives a signal to keep growing. Outdoor light — specifically the intensity and spectral quality of natural sunlight — appears to suppress that growth signal. When kids swap the playground for a screen, they lose that natural brake.
Add in genetics (if one parent is myopic, the child's risk doubles; if both parents are myopic, it quadruples), and you've got a recipe for a myopia epidemic.
How sleepSEE Overnight Lenses Work {#how-it-works}

The concept sounds almost too simple. Your child puts in specially designed contact lenses before bed. They sleep. In the morning, they take the lenses out — and they can see clearly all day. No glasses. No daytime contacts. Nothing.
Here's what's actually happening while they sleep.
The lenses are made of a highly oxygen-permeable rigid gas permeable (RGP) material. They sit on the cornea — the clear front surface of the eye — and apply a gentle, precisely calculated hydraulic force. This temporarily flattens the central cornea, correcting the refractive error that causes blurry distance vision.
But the myopia control part is more interesting. As the central cornea flattens, the peripheral cornea takes on a different curvature. This changes how light focuses on the peripheral retina — the edges of your visual field. In a myopic eye wearing regular glasses, peripheral light focuses behind the retina. That's actually a growth signal — the eye "chases" that focal point by growing longer.
sleepSEE lenses flip this. They create peripheral myopic defocus — peripheral light now focuses in front of the retina. That's a stop signal. The eye stops chasing. Growth slows.
A systematic review published in Ophthalmic and Physiological Optics found that orthokeratology reduces axial elongation (eye growth) by approximately 43–50% compared to single-vision spectacles in children. That's not a minor effect. That's a meaningful intervention.
"In my practice, the kids who respond best to ortho-K are the ones whose parents commit to the nightly routine early. The earlier we start, the more we can protect."
sleepSEE vs. Glasses: Side-by-Side {#comparison}
| Feature | sleepSEE Overnight Lenses | Traditional Glasses |
|---|---|---|
| Corrects daytime vision | Yes — no lenses needed during the day | Yes — but only while worn |
| Controls myopia progression | Yes — reduces eye growth by ~43–50% | No — corrects vision only |
| Mechanism | Corneal reshaping + peripheral myopic defocus | Refractive correction only |
| Wear schedule | Overnight only | All day |
| Reversible | Yes — stop wearing, cornea returns to baseline | N/A |
| Safe for children | Yes — FDA-approved for ages 6+ | Yes |
| Ideal for active kids | Yes — no glasses or lenses during sports | Glasses can break |
| HSA/FSA eligible | Yes | Yes |
When Should You Start? {#when-to-start}

Earlier is better. Full stop.
The rate of myopia progression is fastest between ages 8 and 14. A child who starts ortho-K at age 8 has more years of active control ahead of them than one who starts at 13. The cumulative effect on final prescription — and on lifetime eye disease risk — is significant.
sleepSEE is FDA-approved for children as young as 6 years old. If your child's prescription has changed by -0.50 diopters or more in the past year, that's a flag. Come in. Let's talk.
For a deeper look at whether your child is a candidate, read our guide: Is My Child a Candidate for Orthokeratology? A Complete Parent's Guide [blocked].
You can also explore what the American Optometric Association says about myopia in children for additional context.
Frequently Asked Questions {#faqs}
Are overnight contact lenses safe for children?
Yes. sleepSEE lenses are FDA-approved and made from highly oxygen-permeable materials. With proper hygiene and regular follow-up visits, they are safe for children as young as 6. In my experience, motivated kids as young as 7 or 8 handle them just fine.
How quickly will my child see results?
Most children notice significant vision improvement within the first few days of consistent nightly wear. Full stabilization typically takes 2–4 weeks. Myopia control benefits are cumulative and build over months and years of wear.
What if my child misses a night?
Vision will gradually blur over 1–2 days without wear. It's not harmful, but consistency matters for both vision quality and myopia control. We recommend keeping a spare pair of glasses for the occasional missed night.
Does insurance cover sleepSEE?
sleepSEE® myopia control is a specialty service not covered by insurance. Flexible payment options and HSA/FSA funds are accepted. Contact your sleepSEE provider to discuss payment plans.
Can adults use sleepSEE too?
Absolutely. Adults who want freedom from glasses or daytime contacts — without surgery — are excellent candidates. The myopia control benefit is specific to children (whose eyes are still growing), but the vision correction benefit applies to adults as well.
How is sleepSEE different from LASIK?
LASIK permanently reshapes the cornea through surgery. sleepSEE temporarily reshapes it each night through lens wear. sleepSEE is reversible, non-surgical, and safe for children. LASIK is not recommended for anyone under 18 and is not appropriate for growing eyes.
If your child is squinting at the board, if their prescription has changed in the last year, or if you have a family history of high myopia — don't wait. The window for meaningful intervention is open right now.
Find a sleepSEE-certified provider near you [blocked] and schedule a consultation. Bring the questions. We'll bring the answers.
References
- Holden BA, et al. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042.
- Flitcroft DI, et al. IMI – Defining and Classifying Myopia. Invest Ophthalmol Vis Sci. 2019;60(3):M20–M30.
- Wu PC, et al. Outdoor Activity and Myopia in the Sunlight and Myopia Study. JAMA Ophthalmol. 2018;136(10):1188–1190.
- Charm J. Peripheral defocus and myopia control: a mini-review. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9935061/
Free Download: Myopia Risk Checklist for Parents
Is your child's vision at risk? Get the 10-point checklist used by ortho-k specialists.
- 10 warning signs myopia is progressing
- Questions to ask your eye doctor
- How to evaluate ortho-k candidacy
- What to expect in the first 30 days
Myopia Risk Checklist
For Parents — Free PDF Guide
Dr. James Singletary, OD, FIAOMC
Dr. James Singletary, OD, FIAOMC is a contributor to the sleepSEE Insights blog, sharing expert knowledge on myopia progression, orthokeratology (Ortho-K) and myopia control.