Every week I see the same thing in my Fayetteville practice.
A parent brings in their child — maybe 7, maybe 9 — and the prescription is stronger than last year. Again. The parent sighs. "I figured this would happen. I wore glasses too." And then they ask the question I hear more than any other: "Is there anything we can do to stop it?"
The answer is yes. But most parents don't know that yet. And that gap — between what's possible and what parents know — is exactly why I'm writing this.
Childhood myopia is not just a glasses problem. It's a public health crisis. And here in Cumberland County, we're seeing it up close.
Table of Contents
- What Is Myopia, Really?
- The Numbers Are Alarming
- Why Is This Happening to Our Kids?
- The Long-Term Risks Nobody Talks About
- What Parents Can Actually Do
- Myopia Control Options Compared
- When Should You Start?
- Frequently Asked Questions
- The Bottom Line
What Is Myopia, Really?
Most people think myopia just means "my kid needs glasses." But that's only half the story.
Myopia happens when the eyeball grows too long from front to back. Light focuses in front of the retina instead of on it. That's why distant objects look blurry. But here's what matters most: in children, the eye is still growing. And in myopic children, it often grows too fast, too far.
This is called axial elongation — and it's the root of the problem. Every millimeter of extra growth pushes the prescription higher and increases the risk of serious eye disease later in life.
Standard glasses fix the blur. They do nothing to stop the growth.
The Numbers Are Alarming

The myopia epidemic is real — and it's accelerating. Here's what the data shows:
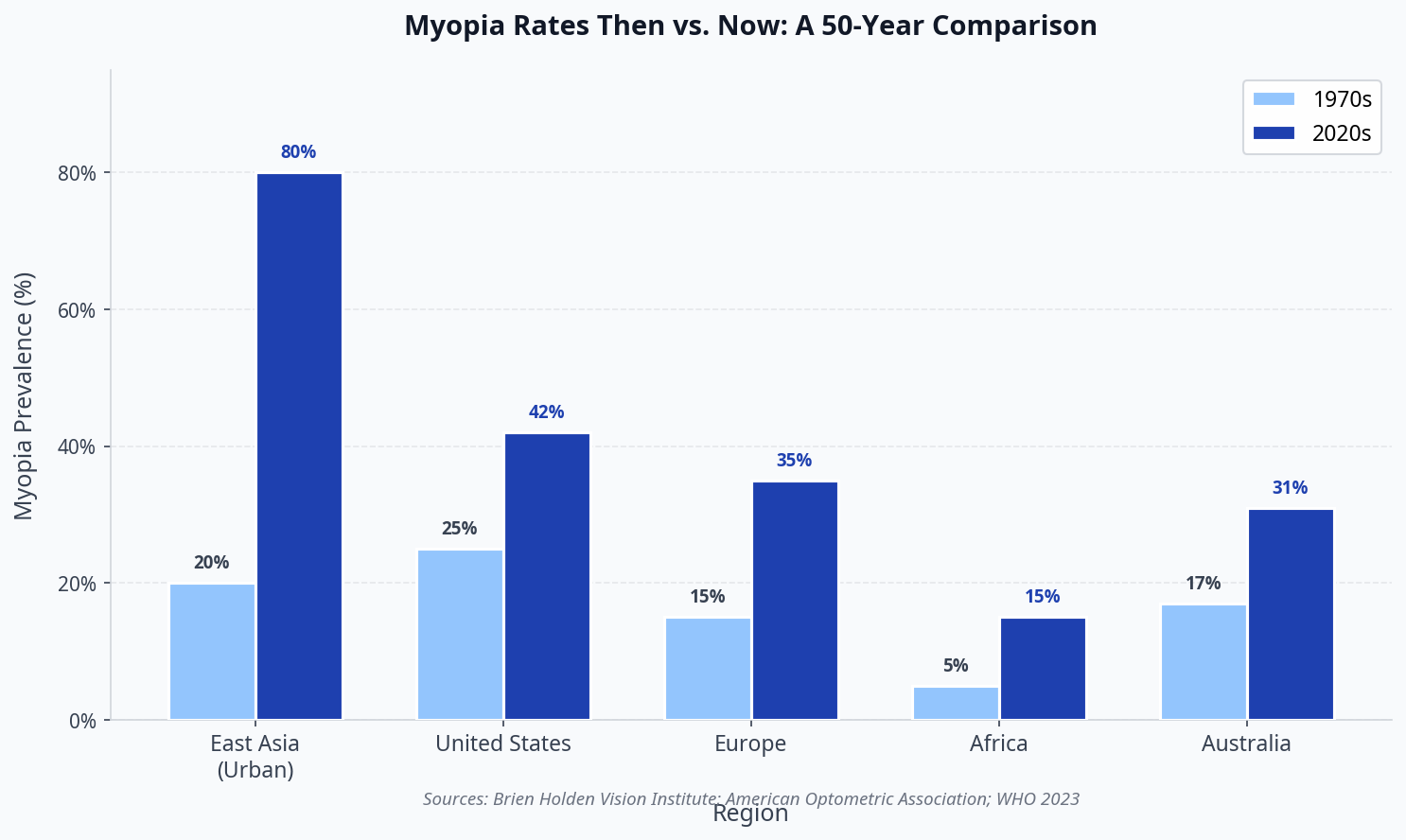
In East Asian cities, myopia now affects up to 80% of young adults — up from roughly 20% just 50 years ago. In the United States, rates have nearly doubled since the 1970s, from about 25% to over 42% today. ¹ ²
Right here in North Carolina, pediatric eye care providers are seeing the same trend. Children in Cumberland County schools — including those connected to Fort Liberty — are presenting with myopia at younger ages and with faster progression than a decade ago.
The Brien Holden Vision Institute projects that 50% of the world's population will be myopic by 2050 if current trends continue. ¹
That's not a prediction. That's a warning.
Why Is This Happening to Our Kids?
Three factors drive the epidemic. None of them are your child's fault.
1. Less time outdoors. This is the biggest one. Natural light — specifically the intensity of outdoor light — appears to trigger the release of dopamine in the retina, which slows eye elongation. Children today spend a fraction of the time outdoors that previous generations did. Studies show that just two hours of outdoor time per day can reduce myopia onset risk by up to 50%. ²
2. More near work. Reading, homework, tablets, phones. Modern children spend unprecedented hours focused on objects within arm's reach. Sustained near focus may contribute to the axial elongation that drives myopia.
3. Genetics. If one parent is myopic, a child's risk roughly doubles. If both parents are myopic, the risk is 6–8 times higher. But genetics alone don't explain a doubling of rates in 30 years — environment is clearly at play.
"We can't change a child's genetics. But we can change what happens next. That's where myopia control comes in."
The Long-Term Risks Nobody Talks About
Here's the part most parents don't hear at a routine eye exam: myopia is not just inconvenient. It's a risk factor for blinding eye disease.
Every additional diopter of myopia increases the lifetime risk of:
| Condition | Risk Increase with High Myopia |
|---|---|
| Retinal detachment | 5–6× higher |
| Glaucoma | 2–3× higher |
| Myopic maculopathy | Leading cause of irreversible vision loss |
| Cataracts | Earlier onset, more severe |
These risks are cumulative and permanent. The higher the prescription climbs in childhood, the greater the burden in adulthood. A child who reaches -6.00 diopters faces a fundamentally different eye health future than one who is kept at -2.00.
That's why slowing progression — even by 40% — can mean the difference between manageable myopia and high-risk myopia.
What Parents Can Actually Do

The good news: myopia progression is not inevitable. We have proven tools to slow it down significantly.
Here's what the evidence supports:
Orthokeratology (Ortho-K) — sleepSEE: Custom overnight lenses that gently reshape the cornea while your child sleeps. In the morning, they remove the lenses and see clearly all day — no glasses, no daytime contacts. Studies show ortho-k slows myopia progression by 36–56%. ¹
Low-dose atropine eye drops: Nightly drops that slow eye growth. Effective on their own, and often combined with ortho-k for enhanced results.
Multifocal contact lenses: Specially designed soft lenses that create peripheral defocus, signaling the eye to slow its growth.
Outdoor time: Simple and free. Two or more hours of outdoor time daily is one of the most evidence-backed interventions available.
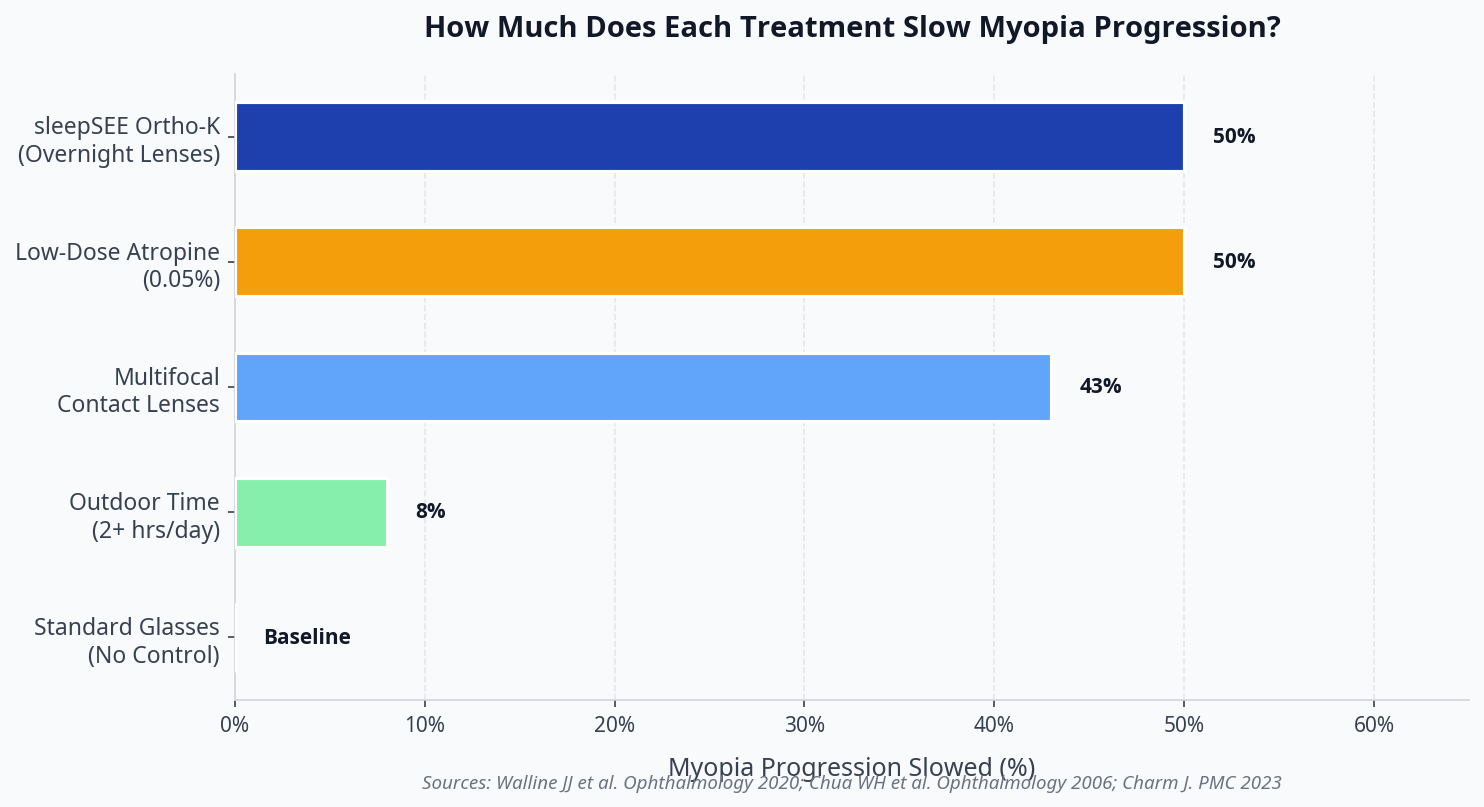
Myopia Control Options Compared
| Treatment | Progression Slowed | Glasses-Free Days | Ages | Notes |
|---|---|---|---|---|
| Standard Glasses | 0% (baseline) | No | All | Corrects blur only |
| Outdoor Time (2+ hrs) | ~8% | No | All | Preventive, not corrective |
| Multifocal Contacts | ~43% | No | 8+ | Worn during the day |
| Low-Dose Atropine | ~50% | No | 5+ | Eye drops, nightly |
| sleepSEE Ortho-K | ~50% | Yes | 6+ | Worn only at night |
sleepSEE ortho-k stands out because it combines meaningful myopia control with the lifestyle benefit of glasses-free days. For active kids — especially those involved in sports, swimming, or military family activities at Fort Liberty — that freedom matters.
When Should You Start?
The earlier, the better. Myopia progresses fastest between ages 6 and 12. That window is when intervention has the greatest impact.
But it's rarely too late. Even a teenager with a -4.00 prescription benefits from slowing further progression. Every diopter prevented is a meaningful reduction in lifetime disease risk.
If your child shows any of these signs, schedule a myopia control consultation now:
- Prescription increases at every annual exam
- Squinting at the board at school
- One or both parents are myopic
- Spending 4+ hours daily on screens or near work
- Less than 1 hour of outdoor time per day

See the chart below for a summary of how each treatment option compares on effectiveness:
Frequently Asked Questions
Is myopia control covered by insurance? sleepSEE® myopia control is a specialty service not covered by insurance. Flexible payment options and HSA/FSA funds are accepted.
At what age can a child start ortho-k? sleepSEE ortho-k is FDA-approved and clinically studied for children ages 6 and up. The earlier a child starts, the more progression can be prevented during the critical growth years.
How long does my child need to wear the lenses? Most children wear ortho-k lenses nightly for as long as myopia is actively progressing — typically through the mid-to-late teen years. Some continue into adulthood for the convenience of glasses-free days.
Is ortho-k safe for kids? Yes. Ortho-k has been used safely for over 20 years. The lenses are FDA-approved, and the corneal reshaping is fully reversible. Studies show complication rates comparable to standard soft contact lenses.
What if my child already has a high prescription? Myopia control is still beneficial. Even at -4.00 or -5.00, slowing further progression reduces the risk of reaching the high-myopia threshold (-6.00+) where disease risks increase sharply.
How do I find a sleepSEE provider near me? Use our Find a Provider [blocked] tool to locate a certified sleepSEE provider in Fayetteville, NC or anywhere in the country.
The Bottom Line
The childhood myopia epidemic is real, it's accelerating, and it carries consequences that extend far beyond needing stronger glasses each year.
The good news: we are not powerless. Proven myopia control treatments — especially orthokeratology — can slow progression by up to 50%, preserve eye health for decades, and give your child the freedom to live without daytime glasses.
If your child's prescription has been climbing, don't wait for the next exam. The window for maximum impact is now.
Find a sleepSEE provider near you [blocked] and ask about a myopia control consultation. Or learn more about how ortho-k works [blocked] and whether your child is a candidate.
Last reviewed: February 2026
References
[1] Brien Holden Vision Institute. "Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050." Ophthalmology, 2016. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5820818/
[2] Vitale S, et al. "Increased Prevalence of Myopia in the United States Between 1971–1972 and 1999–2004." JAMA Ophthalmology, 2009. https://jamanetwork.com/journals/jamaophthalmology/fullarticle/2094947
Free Download: Myopia Risk Checklist for Parents
Is your child's vision at risk? Get the 10-point checklist used by ortho-k specialists.
- 10 warning signs myopia is progressing
- Questions to ask your eye doctor
- How to evaluate ortho-k candidacy
- What to expect in the first 30 days
Myopia Risk Checklist
For Parents — Free PDF Guide
Dr. James Singletary, OD, FIAOMC
Dr. James Singletary, OD, FIAOMC is a contributor to the sleepSEE Insights blog, sharing expert knowledge on myopia progression, orthokeratology (Ortho-K) and myopia control.